
The shoulder joint offers the greatest range of motion of any joint in the human body. This incredible mobility, however, comes at a cost: a susceptibility to wear and tear, injury, and disease. Among the most common and debilitating conditions affecting the shoulder is arthritis. For patients experiencing persistent pain, stiffness, and a loss of function, understanding what causes arthritis in the shoulder, along with the treatment options, is an important step toward effective management.
Key Takeaways
- Shoulder arthritis can develop in several different forms, each with its own underlying cause and progression.
- Arthritis commonly affects two areas in the shoulder: the main ball-and-socket joint (glenohumeral joint) and the joint at the top of the shoulder (acromioclavicular or AC joint).
- Treatment typically begins with conservative, non-surgical methods like physical therapy, anti-inflammatory medications, and injections. When these fail or for severe conditions, surgical options may be recommended.
The Anatomy of the Shoulder
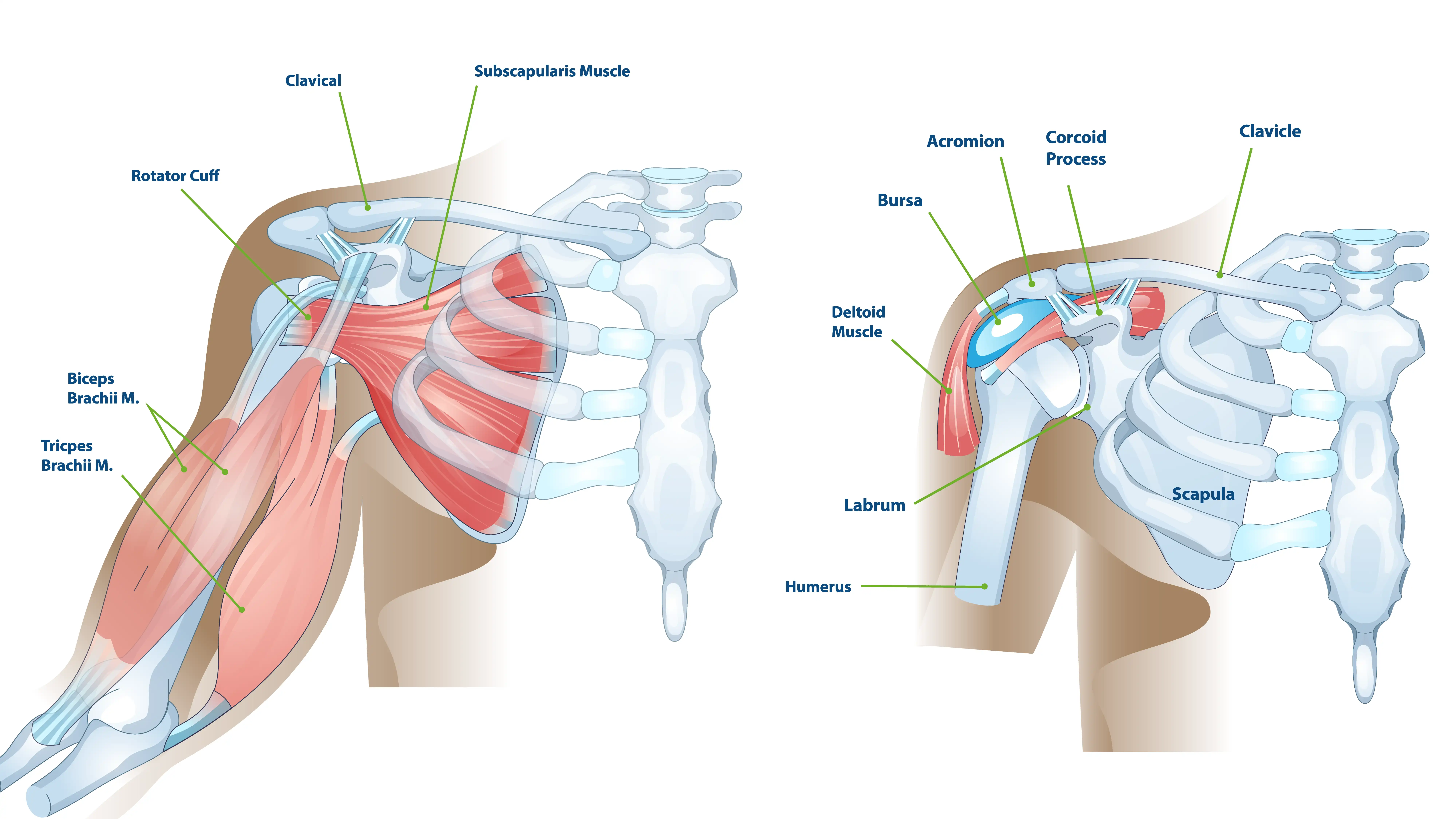
The shoulder comprises three bones: the humerus (upper arm bone), the scapula (shoulder blade), and the clavicle (collarbone). The primary shoulder joint, the glenohumeral joint, is a ball-and-socket mechanism. The rounded head of the humerus (the ball) fits into the shallow socket of the scapula, the glenoid. Articular cartilage, a smooth, resilient tissue, covers the ends of these bones. This cartilage acts as a shock absorber and allows the bones to glide against each other with minimal friction.
A second, smaller joint, the acromioclavicular (AC) joint, sits where the clavicle meets the highest point of the scapula, the acromion. This joint may also develop arthritic changes.
The Primary Causes of Shoulder Arthritis
The causes of shoulder arthritis are diverse, and each type of arthritis has a distinct underlying pathology. In the following subsections, we’ll explore the most common causes of shoulder arthritis.
Osteoarthritis (OA)
We often refer to osteoarthritis as “wear-and-tear” arthritis. It is the most common form of the disease and the primary cause of arthritis in the shoulder. OA is a degenerative condition. It progressively breaks down the articular cartilage. Over years of use, the cartilage softens, frays, and eventually wears away completely. This exposes the underlying bone, which can lead to bone-on-bone friction and bone spur formation.
Risk Factors for Osteoarthritis
While age (over 50) is generally the most significant risk factor, other factors may accelerate the process:
- Genetics: A family history of OA may increase your susceptibility.
- Previous Injury: Fractures, dislocations, or labral tears can disrupt the joint surface, leading to premature wear.
- Repetitive Stress: Occupations or sports involving heavy overhead use (e.g., construction, baseball pitching, tennis) may accelerate cartilage degradation.

Post-Traumatic Arthritis
Post-traumatic arthritis is a form of osteoarthritis that can develop after an injury to the shoulder. Any severe trauma that damages the joint surfaces may initiate the arthritic process. Common injuries that lead to post-traumatic arthritis include fractures and dislocations.
Cuff Tear Arthropathy (CTA)
Cuff tear arthropathy is a severe and unique form of shoulder arthritis that can develop as a direct consequence of a massive, long-standing, and irreparable rotator cuff tear. The rotator cuff muscles stabilize the glenohumeral joint and control the movement of the humeral head within the socket. Cuff tear arthropathy is characterized by the following:
- Loss of Stabilization: When a massive rotator cuff tear occurs and remains untreated, the humeral head can lose its centralizing force.
- Superior Migration: The powerful deltoid muscle, unopposed by the torn rotator cuff, pulls the humeral head upward.
- Joint Destruction: This superior migration causes the humeral head to rub against the acromion (the roof of the shoulder) and the upper part of the glenoid. This leads to destruction of the articular cartilage.
Inflammatory Arthritis (Rheumatoid Arthritis)
Inflammatory arthritis is a group of systemic diseases. The body’s immune system mistakenly attacks its own healthy tissues, including the joint lining. Rheumatoid arthritis (RA) is the most common form affecting the shoulder. Unlike osteoarthritis, which often affects different joints independently, RA typically affects both shoulders simultaneously and symmetrically.
Recognizing the Symptoms
The symptoms of shoulder arthritis usually develop gradually and worsen over time. Recognizing these warning signs early allows for timely intervention and better outcomes.
Pain is the most common and often the first symptom. Many patients describe a deep, aching discomfort in the back of the shoulder that intensifies with activity, especially during overhead movements, and tends to ease with rest. As the disease progresses, pain may become severe enough to disturb sleep.
Stiffness and loss of motion can also develop progressively. Over time, patients may find it increasingly difficult to perform everyday tasks such as reaching for a high shelf, fastening a seatbelt, or combing their hair. Many also experience crepitus, a grinding, clicking, or crunching sound and sensation that results from rough, damaged cartilage surfaces rubbing together.
Weakness commonly accompanies these symptoms. As pain and stiffness limit shoulder use, surrounding muscles gradually weaken from disuse, a process called atrophy. In cases of cuff tear arthropathy, where the rotator cuff tendons are severely damaged or non-functional, this weakness can be severe.
Diagnosis: Pinpointing the Cause
Diagnosis begins with a detailed medical history and a careful physical examination. Your doctor may ask about the onset, location, and nature of the pain, past injuries, and functional limitations. During the physical exam, they may assess active and passive range of motion to determine stiffness and pain, test muscle strength to evaluate the rotator cuff, and use gentle palpation to identify areas of tenderness.
Imaging studies may be used to support the diagnosis and determine severity. X-rays can reveal hallmark signs such as narrowing of the joint space (indicating cartilage loss) and the formation of bone spurs (osteophytes). In cuff tear arthropathy, X-rays may also show the humeral head migrating upward.
When more detailed information is needed, MRI scans can be used to visualize the surrounding soft tissues, especially the rotator cuff tendons, and to detect any large tears that could influence treatment decisions. CT scans provide highly detailed images of the bone structure and may be used before surgery to guide surgical planning.
Treatment Options: A Path to Pain Relief and Function
Treatment for shoulder arthritis frequently begins with non-surgical methods, progressing to surgical options only when necessary. The goal of treatment is to relieve pain, reduce inflammation, and restore mobility and strength.
Non-Surgical Management
The first line of care generally focuses on lifestyle adjustments and physical therapy. Patients may be encouraged to rest from activities that worsen pain, especially heavy lifting and repetitive overhead movements. Applying ice can help reduce inflammation, while moist heat can relax muscles and provide temporary comfort. A structured physical therapy program is important for maintaining range of motion and strengthening the rotator cuff and scapular stabilizers, which support shoulder mechanics and stability.
Medications may also help manage symptoms. Over-the-counter or prescription non-steroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen or naproxen are commonly used to reduce pain and swelling. Acetaminophen may also be taken for pain relief.
In some cases, injections may be recommended. Corticosteroid injections deliver a strong anti-inflammatory medication directly into the joint to offer significant, though temporary, pain reduction. Emerging regenerative therapies such as platelet-rich plasma (PRP) or stem-cell injections show promise in reducing inflammation and promoting healing.
Surgical Management
When non-surgical treatments no longer provide acceptable pain relief or when the loss of function is severe, surgical intervention becomes a possible solution. The choice of procedure depends entirely on the type of arthritis, the patient’s age, activity level, and the condition of the rotator cuff.
Shoulder Arthroscopy
- Procedure: The surgeon uses a minimally invasive technique with a small camera and instruments.
- Indication: Primarily for early-stage arthritis. There are very limited indications.
- Goal: The surgeon removes loose bodies, trims damaged cartilage, and cleans out inflammatory tissue.
Anatomic Total Shoulder Arthroplasty
- Procedure: The surgeon replaces the damaged ball (humeral head) and socket (glenoid) with prosthetic components, replicating the patient’s natural anatomy.
- Indication: Severe glenohumeral arthritis with an intact, functional rotator cuff.
Reverse Total Shoulder Arthroplasty
- Procedure: The surgeon reverses the ball and socket components. They fix a metal ball to the socket (glenoid) and place a plastic socket on the upper arm bone (humerus).
- Indication: Cuff tear arthropathy or arthritis accompanied by a large rotator cuff tear. Other non-arthritic conditions may also indicate reverse shoulder replacement.
- Mechanism: By reversing the ball and socket, the reverse shoulder replacement design relies on the large, powerful deltoid muscle, rather than the non-functional rotator cuff, to power the arm.
Summary
Shoulder arthritis is a complex, progressive condition that can severely impact a patient’s life, but it is often manageable. Whether the cause is age-related wear, a past injury, or a massive rotator cuff tear, a diagnosis is the foundation of a treatment plan. If you experience persistent shoulder pain, stiffness, or loss of motion, consider seeking professional evaluation. Consider consulting with an experienced shoulder specialist to explore a personalized treatment path that will help get you back to the activities you enjoy.
Frequently Asked Questions
Is shoulder arthritis the same as a rotator cuff tear?
No, they are distinct conditions, but they can be related. A rotator cuff tear is a tear in one or more of the tendons that stabilize and move the shoulder. Arthritis is the loss of cartilage in the joint. However, a long-standing, massive rotator cuff tear can cause a specific type of arthritis called cuff tear arthropathy (CTA). You can have both a tear and arthritis simultaneously.
I have a grinding noise in my shoulder. Does that mean I have arthritis?
A grinding, clicking, or crunching sound, known as crepitus, is a common symptom of shoulder arthritis. It may indicate rough, damaged cartilage surfaces are rubbing together. However, crepitus can also result from other issues, such as tendonitis or bursitis.
Can exercise make shoulder arthritis worse?
High-impact or repetitive overhead activities may aggravate arthritis symptoms, but gentle, low-impact exercises are often beneficial. Physical therapy focusing on range of motion and strengthening the supporting muscles can help reduce pain and improve function. Always follow a program guided by your doctor.

